
This is a complementary blogpost to my #smaccDUB talk “How Students Can Choreograph Their Own Education”.
I was thrilled to be offered the opportunity to talk about my passion – medical education, and how I think we can benefit from adding to our current views and knowledge on the topic.
My main take home messages from the talk were:
- Know your educational psychology and theories because with the current approach in medical education we may be creating the exact problems we’re trying to avoid
- Introduce the art of reflection EARLY to start the journey from frustrated, unaware and overconfident novice to flexible, creative and adaptive expert
- Go to the sim like you go to the gym because being an awesome doctor takes training, and training takes time, repetition and reflection
You can check my entire talk below.
Video
Cast
Slides
In this blogpost I’ll try to elaborate in more details on these topics than the above 20-25 minutes at #smaccDUB allowed for.
Behaviourism
I started off by stating that medical education as we know it today is often behavioristic in its approach. And since I’m not a behaviorist I won’t call that right or wrong. But if we only use a behavioristic approach we end up creating learners for whom confidence = competence and we don’t really want that.
Many of the courses we attend both early and late in our career make use of a behavioristic approach. This means it sees learning as applying knowledge to a learner who is treated as a blank slate. The teacher is an instructor that knows what is right and what is wrong and the goal is to condition the learner into “correct” behavior by giving negative feedback (“punishment”) on poor behavior and positive feedback (reinforcement) on good behavior.
A true behaviorist believes that a stimulus will lead to a response, just like Pavlo Skinner and Thorndike did with their dogs, rats and cats.
A true behaviorist doesn’t believe reflection is necessary to learn. Stimulus and response is all that matters. To ensure learning has taken place you instead assess your learner with pre-post intervention assessment; you test and maybe even assess in clinical context by the use of checklists (and if you start thinking about competency based education and assessment right now, this goes for that as well).
Also, in behaviorism the learner is driven by external factors and especially the fear of punishment. In education that is what we know as the fear of failing which is why we know the knowledge of a test waiting at the end of the semester enhances learning.
In the end you trust that the experiences the learners have gained will transfer to other situations.
Does behaviorism work: Yes! and I have nothing against this approach, just be aware of the side effects to it.
The problem
Take a look at the Dunning-Kruger effect below.
Every time you use the stimulus-response you may correct behavior and you may create learners that do as you say. But since reflection isn’t a part of the equation, they don’t know why. They will pass your OSCE, MCQ or assessment, but they don’t know how they did it. They are just trying to please you and avoid failing. As their instructor you will feel “safe” because they have demonstrated the skills in this particular setting. You will give them positive feedback on how they performed in this very specific setting and they will leave feeling very confident and believe you, when you and your test told them, that they are also competent.
You have created a routine expert that thinks that confidence = competence in the real world and pushed your learner all the way up Mount Stupid where the view may be amazing, but there’s a steep and dangerous fall waiting because you didn’t tell them how their newly acquired skill may be challenged (and inadequate) in the real world.

Humanism
Now, let’s say we look at learning from a more humanistic point of view.
Sometimes medical educators think that humanism is in opposition to behaviorism. It is not. It is just a different approach and an approach I also think you can make use of and should know the limitations to.
Students like this approach.

They like it because it allows them to really dive deeply into topics they are interested in. By all means do not kill that intrinsic motivation by thinking humanism is just some touchy-feely stuff. It is not. A central theory in humanism is Maslow’s hierarchy of needs and the belief that learning is about self-actualization. You believe that your learners are on a path to finding and unleashing their true potential and you as their facilitator will try and help them by supporting them in that quest.
Student will learn a lot from a humanistic approach. And they will learn a lot about how they learn and how to find literature on a topic. The challenge of course is to make sure that they will cover the entire needed curriculum based solely on intrinsic motivation. That is probably not realistic ;-).
That is why, just as with the behavioristic approach, we end up with fragmented learning disconnected from prior learning and knowledge and learning that is also disconnected from reality.
And we end up just where we ended earlier: On the top of Mount Stupid.
This time the learners just think they know everything because they think they’ve read and understood everything. They (We!) of course have not.
We should aim to minimize the Dunning-Kruger effect. Not by avoiding the use of the humanistic and behavioristic approaches, but by adding to those.
Constructivism
So many of you may think that the answer is right in front of us with constructivism.
In medicine constructivism is often what we think of as “problem based learning” (PBL)
And PBL does go a long way to try and solve the problem of transfer of learning.
In PBL the facilitator aims to create an environment where the learner can grow and where students construct knowledge via active engagement in their environment. The educator will facilitate use of prior knowledge and experiences and they will ask questions. This is an active learning strategy that requires engagement from both student and teacher. And therefore also requires a lot of the educator in terms of knowledge, self reflection, awareness of own limitations and TIME. Hence, most PBL takes place at the university and not bedside where time and resources are very limited. A constructivist also believes in learning as a process of making “schemes” and since much of the PBL is self-directed and time with the facilitator is limited the challenge is to ensure that existing schemes are connected and combined in the right way. Even though PBL may solve the cognition part of transfer of learning, it doesn’t necessarily bridge from theory to practice in the more complex clinical setting.
The main problem I see with PBL at the moment is that it exists within a behavioristic curriculum where the goal is still right or wrong.
I suggest we need to go beyond constructivism and learn even more about education theory.
First of all: Know your learner!
Connectivism
This has nothing to do with age or “learning styles” (I met many non-millennials, reflectionists and introverts at SMACCDUB who were still learning through social interaction ;-)), but everything to do with realizing that the curriculum in medical school and beyond is probably too narrow-minded.
Instead, I would love to see learners of all levels involved in curriculum design. Allow for, and encourage engagements outside the curriculum and recognize that searching for literature and finding knowledge and answers are also a core skill for a future excellent doctor.
Get familiar with connectivism and use it to encourage your learners to “connect” as well. With each other and #FOAMed.
Encourage the development of personal learning networks through twitter, blogs, and other social medias, and realize that critical appraisal is something they should train and learn also in the online and social environment.
So if we want our learners to move from unaware, frustrated, under-competent and overconfident fools towards creative, flexible and adaptive experts we need to aim for adaptive expertise in medical education.
How do we do that?
Adaptive expertise
Take a look at the curve by Daniel Schwartz and colleagues from Stanford on transfer of learning below.
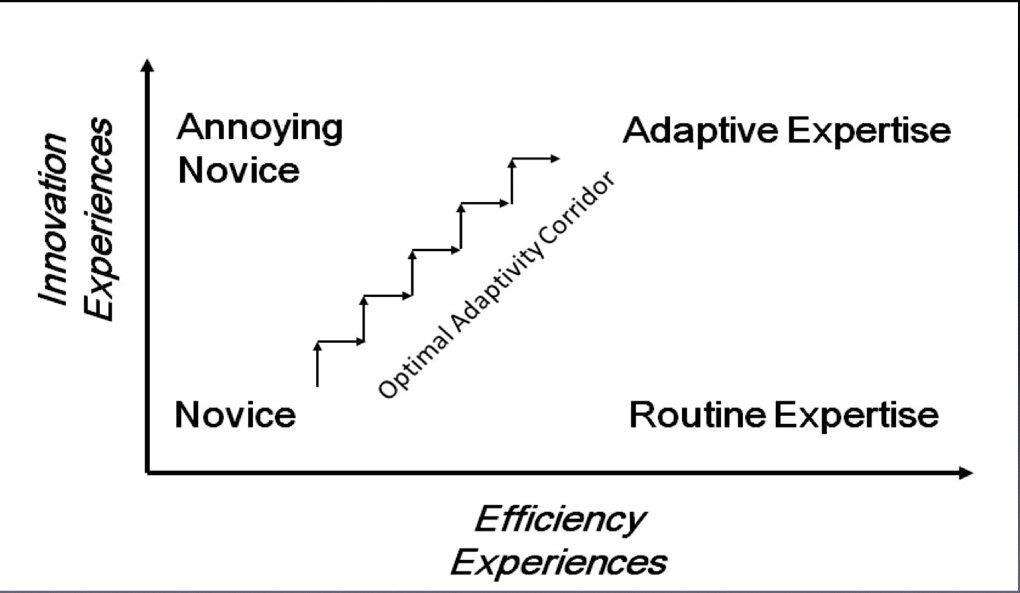
Now if we put it on top of the Dunning-Kruger then we might explain the process something like this.

Aim for adaptive expertise by walking in the optimal adaptivity corridor. Adaptive expertise is not something we are particularly familiar with in medicine. A simplified suggestion might be to provide and allow for the following three fundamental principles
- Question everything!
- Reflect to facilitate deeper learning
- Train in a minimal-risk or risk-free environment
When you do that, you walk hand in hand with your learner up Mount Stupid in small steps and, just when they feel confident, you challenge them on their believes. You make them reflect, you question their assumptions, you have them challenge each other, yourself and and everyone they meet. They learn that confidence does NOT equal competence in all situations. They learn that their solution to the problem is not the only one. They learn that there is more than one solution to every problem (even when an algorithm is involved!) and that other people’s experiences may add value to their toolbox for future use.
That way you end up moving in little steps in the adaptive corridor. Instead of rushing up Mount Stupid.
So educate your learners where you make use of all educational theories. Train your learners. By all means assess and correct and inspire and support interests. But on top of that REFLECT.
SIM like you GYM
The third suggestion in adaptive expertise is also training in a risk-free environment and that’s why I introduced the “Sim Like You Gym” that quickly found it’s way to twitter as a bit of a meme:
Open up the sim centers and other training environments where training is low-risk or preferably completely risk-free. And I mean really open up. In terms of accessibility, “opening hours” and the faculty. Invite students into your faculty, you may end up training their reflective skills from early on and end up with some very skilled educators to recruit from to future projects and positions. Not a bad side effect.
Involve students in your faculty! Where I work, at Copenhagen Academy for Medical Education and Simulation, we do just that. Students have developed a course on patient safety for the Copenhagen med schoool. They do peer-to-peer teaching, teach resuscitation guidelines to peers and non-peers, develop ultrasound apps and participate with many functions in simulation training as operators/technicians, standardized patients, confederates in scenarios etc.
Our simulation center is open to the students’ own educational initiatives, for instance research or courses developed by students for students in their spare time. Courses in surgical skill training and emergency medicine and procedures have been designed by students and run for years, to allow students to take responsibility for their own education.
Involve students in choreographing their own education and know and appreciate that education takes time and practice. And requires spaced repetition.
So “Sim Like You Gym”: Do a “cardio” class on Monday, kettle bells for your brain on Wednesday (maybe do that one everyday!) and “pulmonary” class on Fridays.
End each sessions with reflection and debriefing and stop thinking that more scenarios will do the trick. It’s in the reflection in the debrief that the real learning takes place.
So by going to the sim like you go to the gym. You repeat and refine. You build “muscles” by training your cognition, by making new patterns and connections in your brain. You find out many new solutions to the same problem and you train in different teams with different people.
This increases and develops creativity and flexibility and of course makes you an adaptive soon-to-be expert.
Warning!
Side effects: Plenty..…If you train repeatedly with different team members you may expand your network, gain new friends and help reduce tribalism!
Finally – Thanks for all the feedback from friends and new friends on my talk. I enjoyed giving this talk with you as my audience and every single tweet, comment and email has meant a lot! See you at #dasSMACC.
Vb
Sandra
References:
1: Kawamura A, Mylopoulos M, Orsino A, Jimenez E, McNaughton N. Promoting the Development of Adaptive Expertise: Exploring a Simulation Model for Sharing a Diagnosis of Autism With Parents. Acad Med. 2016 May 31. [Epub ahead of print] PubMed PMID: 27254013.
2: Koh GC. Revisiting the ‘Essentials of problem-based learning’. Med Educ. 2016 Jun;50(6):596-9. doi: 10.1111/medu.12794. PubMed PMID: 27170074.
3: Goldie JG. Connectivism: A knowledge learning theory for the digital age? Med Teach. 2016 Apr 29:1-6. [Epub ahead of print] PubMed PMID: 27128290.
4: Kay D, Kibble J. Learning theories 101: application to everyday teaching andscholarship. Adv Physiol Educ. 2016 Mar;40(1):17-25. doi:10.1152/advan.00132.2015. PubMed PMID: 26847253.
5: Weidman J, Baker K. The Cognitive Science of Learning: Concepts and Strategies for the Educator and Learner. Anesth Analg. 2015 Dec;121(6):1586-99. doi:10.1213/ANE.0000000000000890. Review. PubMed PMID: 26579660.
6: Flynn L, Jalali A, Moreau KA. Learning theory and its application to the use of social media in medical education. Postgrad Med J. 2015 Oct;91(1080):556-60. doi: 10.1136/postgradmedj-2015-133358. Epub 2015 Aug 14. PubMed PMID: 26275427.
7: Mylopoulos M, Woods N. Preparing medical students for future learning using basic science instruction. Med Educ. 2014 Jul;48(7):667-73. doi:10.1111/medu.12426. PubMed PMID: 24909528.
8: Brooks MA. Medical education and the tyranny of competency. Perspect Biol Med. 2009 Winter;52(1):90-102. doi: 10.1353/pbm.0.0068. PubMed PMID: 19168947.
9: Schwartz, D. L., Bransford, J. D., & Sears, D. A. (2005). Efficiency and innovation in transfer. In J. Mestre (Ed.), Transfer of learning from a modern multidisciplinary perspective (pp. 1-52). Greenwich, CT: Information Age Publishing.

Star skater, simulationista by day, anaesthesia by night and #meded choreographer. Coming to a SIM room near you. With a shark.
Reflective practice is essential but creating the conditions for it to occur is more difficult!
Successful learners just seem to know how to move through Kolb’s cycle: experience > reflection > abstraction > experimentation.
Others just stay in the concrete phase trying to parrot the lessons from one discrete experience to the next.
Hi Derek,
Thanks for commenting. Maybe reflective practice is born out of educators asking the right questions and thereby teaching learners how to move through and build bridges between the different steps of Kolb’s ?
And spot on with the “parroting” …that is probably the behaviorism with no reflection upon it that let learners to think that if A worked under X it probably also works under Y Z and so on.
/Sandra
Or maybe under-performers simply can’t find their way? I think Kolb’s circle describes when it works? maybe not so much how to make it happen when learners struggle?
I think the current research in psychology tells us that successful learners are better at self-assessment, better at knowing their limitations and have better insight in own flaws and shortcomings. The landmark paper from 1999 by Dunning-Kruger and the more recent paper from 2008 by the same have some interesting takes on this topic.
And so of course does all the literature on deliberate practice and adaptive expertise.
/Sandra
Thanks for posting
Agree I previously have made the mistaken assumption that by the time a doctor graduates from university they would have developed mature learning techniques. Over time I have found this is the exception rather than the rule. Many of the techniques decribed in the book, ‘Make it stick’ such as generation, elaboration, retrieval practice and deliberate practice are rarely employed in their own time. I have now decided to incorporate more of these exercises in teaching sessions so that they can understand how to apply this at home. Clearly this comes at the expense of pure content delivery but hopefully… Read more »