
In June I had the great pleasure of speaking at one of the most exciting recent conferences for paediatrics: DFTB19 in London. I was invited to talk about virtual reality (VR), based on my research on how 360 degrees videos can be used in paediatric first aid courses, and my involvement in medical education at Copenhagen Academy for Medical Education and Simulation (CAMES).

Just the other day my talk was released on the DFTB website – watch or re-watch my talk by clicking on the picture above.
Some time has passed since the conference and that time has allowed for some reflection, so I thought I would supplement my talk with this blog post. Below you will find a more in-depth walk-through of the main messages from my talk, with some added reflections and comments, and at the end my reflections after receiving my feedback from the audience and the DFTB team. My talk featured a Peter Pan theme also visible in this post. Enjoy!
The Problem
Many innovative people have worked hard on improving CPR training and outcome throughout time. For a short history of resuscitation innovation and education watch this short video where I take you through the early and more bizarre methods of resuscitation up until today’s more advanced interventions.
However, even though we have come a long way, there are still things we can tweak to ensure flexible, repeatable, motivating and safe CPR training to further improve patient outcome from cardiac arrest.
Current literature mentions several challenges in today’s CPR training (1). For instance, it is acknowledged that current training encounters barriers in the form of logistical problems, transfer of skills, and knowledge issues, limited time for training, performance anxiety issues, and the fact that skills decay faster than course participants attend new courses. Together, that presents a threat to the goal of delivering optimal care to our patients at all times.
To reduce some of these challenges, we should consider and harness the potential of new technologies such as virtual reality (VR) and augmented reality (AR).

And so, the aim of my talk was to give the participants an idea about where and how AR and VR are used in today’s resuscitation training and try to facilitate creative ideas on how we can use these new technologies to bridge the gap between classroom training and real life emergencies.
Augmented Reality in today’s CPR training

AR describes display-based systems that combine the real world with virtual images, that are interactive in real time and register the real-world environment (2).
One example of AR is Pokemon go where you are able to see the real world through your smartphone, but with overlaying virtual information, in this example a virtual pokemon.
More advanced AR systems often use a head mounted display, or goggles. Mixed reality (MR) also covers the AR spectrum and can basically be considered as a larger class of technologies that covers augmented reality and virtuality (3).
For more info on AR as a technology read this short review on the topic (open access) (4).
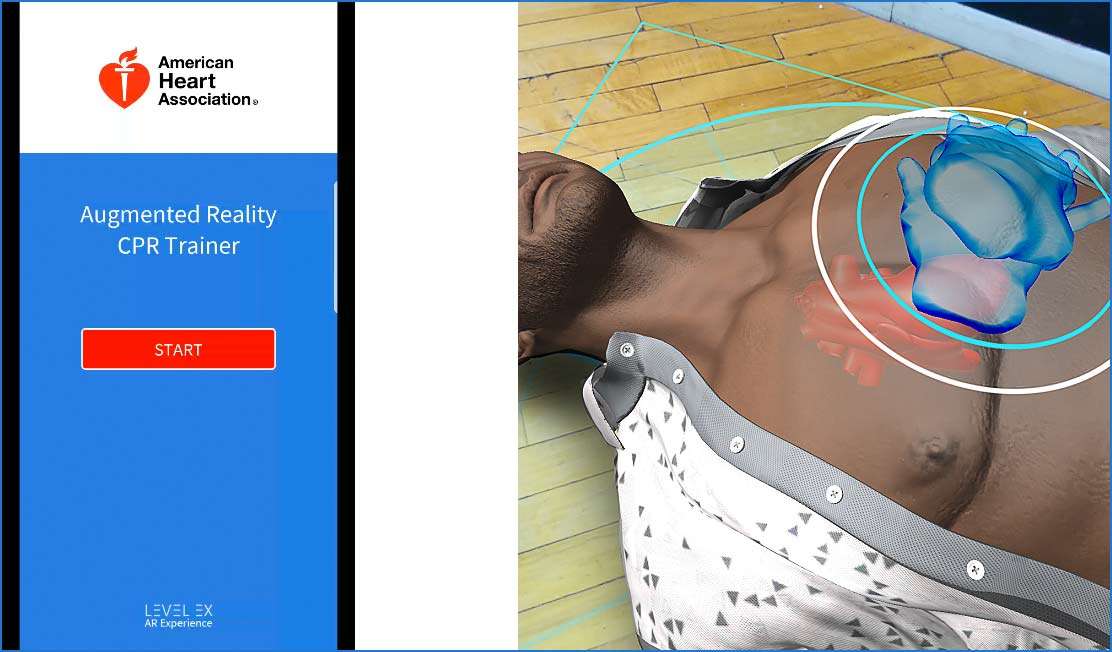
The American Heart Association has launched an app that aims at improving CPR ability which represents a new avenue for delivery of heart health information to the public. Players are scored and rated on how well CPR is performed, including delivery of chest compressions at the correct rate and depth. This technology combines gaming and skills training, introducing laymen to save lives using CPR.
The My Cardiac Coach app with the AR aspect is available for download on Android devices. Watch a demonstration here:
Another example of an AR product that can train CPR performance is Brick simple’s CPReality. Here blood flow activity to the heart, lungs and brain are demonstrated to the participants in the head mounted displays. The system saves the simulation metrics and gives the participant feedback. The AR application is developed for the Microsoft HoloLens and integrated with a CPR manikin.
The Microsoft Hololens uses a big scale AR technology, often referred to as MR. The Hololens has been used in different areas of medical education, for example combined with the LucinaAR technology in obstetric scenarios, where you can see the manikin in the real world through the glasses, but also a virtual fetus which enables you to visualise different birth scenarios and allows you a visual understanding of complication risks and how to act.
This technology adds a whole new layer to our already well-established mannikin training.
Virtual reality in CPR training

In VR you are completely immersed in the virtual world and the real world is blocked out. The simulated experience can be similar to or completely different from the real world; in any case fidelity comes through immersion (5).
With VR you can obtain a sence of really being there, described as presence (6). The feeling of presence provides a possibility for experiential learning, which can lead to enhanced learning effect (5).
VR, like AR, comes in a wide spectrum ranging from really simple 360 degrees film where you are not able to interact with content, to fully immersed VR where you can control a scenario, interact and perceive different inputs as sound, visual and haptic feedback, and even smell and taste.

In 2017, we (CAMES and Child Life) created three 360o movies to describe different scenarios in addition to hands on manikin training in pediatric basic life support courses for laymen.
In a randomised controlled pilot study 52 student teachers were randomised to an intervention group exposed to 3600 movies in training or a control group with traditional training. The three movies included the following themes: CPR, foreign body airway obstruction and convulsions.
Our article is not yet published, but a 360 degree presentation of the project can be found here (7).
Also, the abstract from IPSSW 2018 can be found here
The resuscitation council in the UK has created an interactive way to engage and teach young people CPR. With the lifesaver VR app, participants are presented to a scenario where a young man suddenly goes into cardiac arrest. The participants then have to choose how they will act to questions asked throughout the scenario.
To get started with this type of training you only need a smartphone and a simple cardboard box as a head mounted display which costs around 6-10 euros. Given that, you can train anywhere, at any time, removing some of the barriers to training mentioned earlier.

But multiple, more advanced VR systems for CPR training and other high stake, low frequency events are on the market.
One example is Dual Good Health that has VR content for basic, advanced and paediatric life support.

Another example is the content from Oxford medical simulation which includes virtual reality pediatric and acute care simulations.
A third is the immersive enviroment created at Childrens Hospital of Los Angeles (CHLA) which simulates conditions that might be experienced by junior doctors, when they see acute paediatric patients.
Practice what you preach
When one of your dreams is to ensure motivating educational content, and your passion is innovation, then of course you should consider bringing these parts into you talk as well.
For my talk in London I had teamed up with a company called Rokoko that has specialised in accessible and affordable motion capture suits used in gaming, education, sports, health, films, live performances, and VR/AR experiences. In collaboration with Rokoko we developed a small demo that showed how a motion capture suit, live, can track participant moves and be integrated in CPR training. The dream is for this technology to be combined with head mounted displays allowing the VR-participants to see their own extremities, but also other co-participants and their live movements.
This will allow us to create content where participants can interact with each other in a virtual environment without necessarily being at the same physical place. Participants will be able to be a part of a scenario very similar to real life, but without being in a real emergency situation or even in a sim center.
Furthermore, the program saves all the recordings which allow you to do a short replay where you can zoom in on specific details and shift perspective which is a huge advantage compared with traditional video recordings in 2D. This feature can of course be used in debriefings after a scenario
Information about the smartsuit can be found here: Rokoko smartsuit pro


Both photos ©Ian Summers
Limitations and advantages

AR and VR offers a lot of opportunities, but we still face some limitations.
Both new technologies have survived the introduction phase in medical education and also in the CPR area of resuscitation training. Both AR and VR content have shown huge potential and I think that both, without any doubt, will be a permanent part of the future healthcare education content and also have a role in CPR training programs.
As with any new technology it is important to assess the true value of the new systems and make sure that we use our resources in the best way. This requires valid and high-quality research in the area which is still lacking.
Good and high-quality hardware is still expensive, but compared to high fidelity manikins and full-scale simulations it is affordable for many institutions. Using the wrong equipment and hardware or having the content developed by an inexperienced developer can result in issues as cybersickness (the bodily discomfort you can experience when using VR systems) which will affect the participants learning experience.
Development of content is time consuming and requires software developers, producers, and programmers. In the future we should consider sharing content between institutions.

The list of advantages is long, but some of them includes:
Repeatable scenarios – which allow us to practice as much and as often as we find it necessary.
Flexible training – most systems can be used anywhere, at any time to integrate simulation with everyday practice. Just imagine having a virtual lab at your hospital, that you can visit if you have an extra hour during the day.
Dr Joyce Yeung et al. compared the effect of VR training only, face-to-face training only, and a combination of VR and face-to-face training (8). They found comparable learning outcomes for several key elements of successful CPR and concluded that VR training could be considered when resources or time doesn’t allow face-to-face training. They also concluded that the real benefits of VR CPR training with the Lifesaver app could be realised if paired with face-to-face training as we did in my Child life 360 video project mentioned earlier.
Feedback – it can provide immediate, objective and personalised feedback.
The future
Many exiting things will happen in this area over the next years as development in this field is fast. As new technologies evolve and become more affordable, we must consider how to use these systems in the best way and how to measure and evaluate the effect. But we cannot do this alone…

Cooperation between tech developers and medical personal to ensure the right educational content delivered in the most effective way is crucial.
Let us team up and see where this new technology era brings us.
And as said in Peter Pan; “All you need is faith, trust, and a little pixie dust.”
After Don’t Forget the Bubbles 2019
Feedback time. From the day you are accepted as a speaker at DFTB you are part of an amazing experience. Before the conference you are offered feedback on slides and content and you’ll receive a lot of useful information which especially helps a newbie like me. But even after the conference the learning experience for me as a speaker continued.
I was very fortunate to receive feedback on my talk, and for all of you present, thank you for the feedback and for taking the time to write both appreciative feedback and suggestions for future things to include. Interestingly, the coaching part of the feedback I received aligned very well with what I was thinking in the days following my talk.
The main question I got was: “How do we get started using AR/VR when we go back home”.
After some thought, here are 9 things I suggest you consider when wanting to start implementing AR/VR in your curriculum.
Step 1
Consider the learning challenge. What are the learning objectives? What complicates the learning without the use of AR/VR? What can AR/VR help with – define the exact challenge!
Step 2
How much time do the participants have for learning, including getting the AR/VR system ready.
Step 3
How should feedback be provided to the participants? Direct in the AR/VR app? By peers? By instructor/teacher? And consider what feedback from Ar/VR systems are capable of and useful for.
Step 4
Selecting the right system/hardware/app etc. Are you able to find an already existing programme for your challenge or should you create new content?
Step 5
If you need new content; team up with professional developers/programmers or existing corporations specialised in this field. Create a VR storyboard template to make sure that they captures your ideas for a scenario/etc.
Step 6
Create the right information for participants and educators. Purpose for learning, learning goals, focus point, how to use the technology, how to receive feedback and why they are being introduced to this new learning style.
Step 7
Educate teachers/facilitators in the technology. How to use the equipment, how to manage system breakdown and so on.
Step 8
Consider availability in order to ensure flexibility and repeatability for the learners. Should they be able to train at home? Could you provide them with a VR-lab on wheels? Open access VR lab in your sim center?
Step 9
Have fun and please share your experiences in the comments below and with the whole world.
Further reading
Letter to the editor. Virtual reality cardiopulmonary resuscitation (CPR): Comparison with a standard CPR training mannequin.
Thank you!
A huge thank you to the amazing Don’t Forget the Bubbles team for always ensuring high quality content on your webpage, exciting and giving conferences and your never-ending passion.
Camilla
References
1. Braslow A, Brennan RT, Newman MM, Bircher NG, Batcheller AM, Kaye W. CPR training without an instructor: development and evaluation of a video self-instructional system for effective performance of cardiopulmonary resuscitation. Resuscitation. 1997;34(3):207-220. doi:https://doi.org/10.1016/S0300-9572(97)01096-4
2. Azuma R, Baillot Y, Behringer R, Feiner S, Julier S, MacIntyre B. Recent advances in augmented reality. IEEE Comput Graph Appl. 2001;21(6):34-47. doi:10.1109/38.963459
3. Milgram P, Colquhoun H. Chapter 1 A Taxonomy of Real and Virtual World Display Integration.
4. Kamphuis C, Barsom E, Schijven M, Christoph N. Augmented reality in medical education? Perspect Med Educ. 2014;3(4):300-311. doi:10.1007/s40037-013-0107-7
5. Kwon C. Verification of the possibility and effectiveness of experiential learning using HMD-based immersive VR technologies. Virtual Real. 2019;23(1):101-118. doi:10.1007/s10055-018-0364-1
6. Heeter C. Being There: The Subjective Experience of Presence . Presence Teleoperators Virtual Environ. 1992;1(2):262-271. doi:10.1162/pres.1992.1.2.262
7. Sørensen C, Hasselager A, Sonne M, Dieckmann P. Use of 360 degree movies in paediatric emergency courses for laypersons. https://www.thinglink.com/mediacard/1050304742879657985
8. Yeung J, Kovic I, Vidacic M, et al. The school Lifesavers study—A randomised controlled trial comparing the impact of Lifesaver only, face-to-face training only, and Lifesaver with face-to-face training on CPR knowledge, skills and attitudes in UK school children. Resuscitation. 2017;120:138-145. doi:10.1016/j.resuscitation.2017.08.010

MD, Tourette's disease researcher, wee enthusiast.